Introduction
One of the questions we’ve been getting frequently over the last year has been “What do we think about peptides?” If you use social media, you’ve likely heard about them, if not seen them promoted. As of May 2026, there are over 700,000 posts on Instagram with #peptides, and over 270,000 on TikTok. They are being touted in the wellness space for a wide array of benefits, from skin health to healing after injury to longevity. There are articles addressing their recent rise in popularity in Time, NPR, and CBS News. They are currently being given at some med spas, physician offices, and wellness clinics. Most of these are IV or injection treatments, as most peptides are degraded in the stomach and are not orally bioavailable.
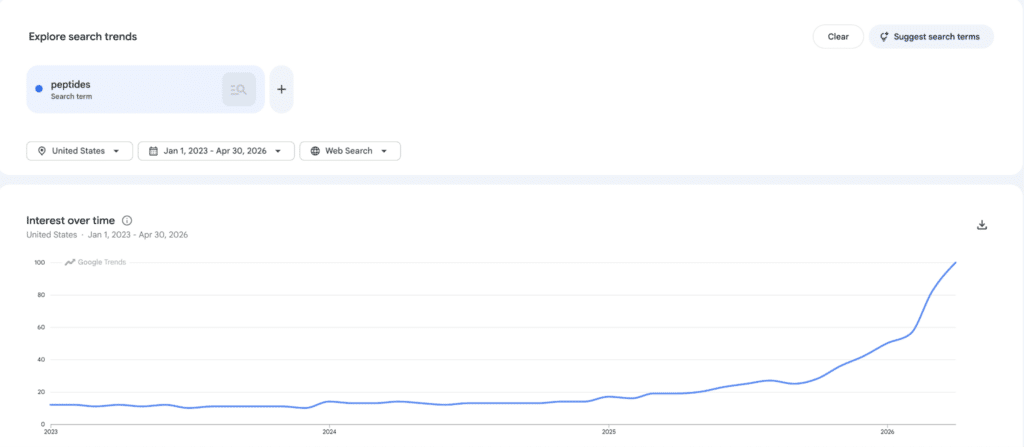
This graph clearly shows the rapidly increasing use of the search term “peptides” on Google.
Today I’d like to address what peptides are, why we’re hearing more and more about them, and then look at how we might evaluate their use, safety, and potential benefits. My goal is not to make an argument for or against them, but rather to shine a light into what is known about these treatments. So far, our answer to the question above has been that we just don’t have enough information. But given the rising popularity, I think it’s important to look at what information we do have. The post is a little long, and at times technical. But I didn’t see any other way to treat it justly. The subject is genuinely complex, so feel free to focus on the sections most relevant to you.
What Are Peptides — And Why Is Everyone Talking About Them?
What Are Peptides and How Do They Work in the Body?
The term peptide refers to a short chain of amino acids, typically between 2 to 50. Amino acids are the building blocks of proteins. So a peptide is really just a very small protein. Peptides aren’t new, and there are naturally occurring peptides that you are probably already familiar with, like insulin and endorphins. Peptides can be signaling molecules that your own body makes, like insulin, or they can be synthetic and used as medications. Ozempic (semaglutide) and Mounjaro (tirzepatide), two medications used in diabetes and weight loss, are both chemically modified peptides. Now we know why the names end in “tide!” But when people are discussing “peptides” in the wellness space, they are generally referring to a group of experimental peptides that have not been FDA-approved, but are believed to have the potential for health benefits. These have names like BPC-157, TB-500, and CJC-1295 to name a few. They are often combined and offered as a blend or “stack” with names like “Wolverine Stack,” or “GLOW Stack,” for example. The purported benefits can be recovery from injury or workout, anti-aging, improving skin health, rejuvenation, improving performance, and cellular repair.
Why We Can’t Just Take Wellness Claims at Face Value
Do Peptide Therapy Benefits Have Real Scientific Backing?
With potential benefits like those, it’s easy to see why there is so much interest in these treatments. The key word in the last sentence, however, is “potential.” We’ll get to that shortly. Interest in these treatments is fueled as well by the lack of FDA-approved medications for most of these goals or conditions. For example, we have no known medication that will improve how quickly a person recovers from a hamstring strain, nor from a torn rotator cuff tendon. In addition, the excitement around peptides is amplified by the modern-day promotion machine that exists on the internet in the form of social media and content creators. I don’t mean this in a negative way. Many of the sites that promote them will also say that they are experimental. There are also influencers who speak about caution, and ask people to become educated before considering a treatment. The difficulty comes when watching a well-made video or reading a well-written account of someone who feels like they were healed or greatly improved by a peptide treatment. The stories can be quite compelling. In addition, some people are hearing from friends or colleagues that a treatment helped, or that they heard about athletes that use them regularly. This type of information or evidence is hard for an individual to evaluate.
Part of the difficulty is that we never get to reverse time and see if someone heals without the treatment. Many people recovering from an injury are also doing other things as well, like physical therapy for example. With skin treatments, peptides may be given at the same time as other therapies, and it may not be clear which therapy worked. There is also the placebo effect, which is stronger for injections than for pills, and which has the ability to confound even the most discerning minds!
How Medicine Actually Evaluates New Treatments
What Does Evidence-Based Research Say About Peptide Safety?
For these reasons, the vast majority of medicine follows an evidence-based practice. There is a general path, that goes from supposing a substance might be beneficial, followed by a process of benchtop laboratory testing, then potentially animal-based studies, phased clinical trials that look at safety and efficacy, randomized controlled trials that involve comparison to a known effective medication or placebo, and finally post-marketing surveillance for data on real-world safety and efficacy. The primary supposition may have come from the chemical’s mechanism of action, or the discovery or creation of something that is similar to a known effective medication. The whole process is cumbersome, but most physicians and scientists agree that it’s necessary to really know if something works or not. It’s even more important when looking at treatments that we REALLY want to have, like improving athletic recovery or performance, having more youthful skin, or living longer. The English philosopher Sir Francis Bacon said it well in 1620, “Let every student of nature take this as a rule: that whatever his mind seizes and dwells upon with peculiar satisfaction is to be held in suspicion; and that so much the more care is to be taken in dealing with such questions to keep the understanding even and clear.”
With that as a background, let’s look at a few of the most commonly given peptides, and see what scientific evidence we do have. Let’s look at the GLOW stack and review the 3 peptides that it usually contains, GHK-Cu, TB-500, and BPC-157. We’ll look at what they are, and what evidence we have to support their use.
GHK-Cu: An Interesting Discovery With Incomplete Evidence
GHK-Cu Peptide Benefits, Research, and Lack of Human Trial Data
GHK-Cu is a 3-amino acid peptide complexed with copper. It was discovered in the 1970s by Loren Pickart during an experiment where he was looking for factors that when added to older liver cells made them behave like younger cells in culture. GHK has a high affinity for copper, and copper is involved in some enzyme reactions related to tissue healing. Plasma levels of GHK also decline in humans as we age. So the beginnings of this story make sense, as it was discovered through a logical experiment on aging biology. The original research by Pickart is not available online, and subsequent review articles are almost all written by Pickart himself, and cite his earlier work, but don’t provide any new experimental data. In spite of this, his claims have become more expansive in articles from 2008 through 2018. In his 2018 review article he claims that GHK-Cu is helpful in wound healing, as well as being anti-cancer, anti-anxiety, anti-pain, helpful in lung disease, and involved in DNA repair. Pickart’s reviews also reference studies showing cosmetic efficacy, and it is currently being used in some skincare products. Those studies, however, are unpublished, and appear to be proprietary company reports or data.
Fortunately, we do have some independent research on GHK-Cu by a group in France in a 1993 study in the Journal of Clinical Investigation. Using a rat wound model, they showed that GHK-Cu produced a dose-dependent increase in wound dry weight, protein, and collagen. They did have a control that was a different 3-amino acid peptide without the copper that did not produce any effect. While this was a well-done study and did show an effect, there are some limitations. Note that this was a model, and not an actual wound. It was done in rats, and not humans. It’s also not clear that an increase in wound dry weight, protein and collagen is equivalent to better wound healing.
Rather than go into detail on the rest of the independent research, I’ll just list the following studies here:
- Wang et al. in 2017 in China showed that GHK-Cu applied topically to mice shortened the healing time of a scald wound.
- Ma et al. in 2020 in China showed that GHK-Cu slowed lung scarring in a mouse lung-scarring model.
- Deng et al. in 2023 showed that GHK-Cu could protect against cigarette smoking-induced skeletal muscle dysfunction in mice with lung disease.
So that’s the summary of what is known scientifically about GHK-Cu as a therapeutic agent. Note that we don’t have ANY human data on its use as an injectable, which is how it is currently used in the ‘peptide’ landscape.
My summary of the above is that Pickart discovered a genuinely interesting molecule in 1973, and published a small amount of original data in the 1970s and 1980s, but since then his research has mainly been reviews that reference his prior work, and his focus appears to be on commercialization. Why has more research on GHK-Cu not been done? For one thing, it is not easy to patent as it’s a naturally occurring substance. This means that the pharmaceutical industry is not as incentivized to study it. Also, for cosmetics, there is no regulatory requirement to prove efficacy. It’s also possible that some trials may have been done that didn’t show a beneficial effect and weren’t published. From the available data, it’s easy to see why GHK-Cu is not an FDA-approved drug for any indication. It simply has not been shown to be safe or effective as an injected medication.
The next peptide to look at is TB-500.
TB-500: A Synthetic Fragment Built on Borrowed Reputation
TB-500 Peptide: What the Research Actually Shows
TB-500 is a synthetic version of a 7-amino acid fragment of thymosin beta-4 (Tβ4), a 43-amino acid peptide found in nearly every cell in the body. Tβ4, the parent peptide, is naturally occurring and is felt to be involved in migration of cells and repair of tissue. It “sequesters,” or keeps a structural protein called actin available for use if needed by your cells. After injury, Tβ4 appears to be released by platelets and immune cells, and is suspected to help coordinate or help with repair or remodeling at the site of injury. Of note, TB-500 and Tβ4 are not the same thing. TB-500 is synthetic, and is just a small fragment of Tβ4.
TB-500 appears to have emerged commercially in the equine/performance world by the early 2010s. It was later banned by WADA, the World Anti-Doping Agency (and the horse racing industry).
Interestingly, however, we have very little published data on TB-500. The vast majority of the literature on this subject is about Tβ4, which is a very different molecule. I think many people incorrectly assume that data on Tβ4 can be transferred over to TB-500.
The Tβ4 data is reasonably strong. Multiple independent groups have shown that Tβ4 accelerates wound healing in various animal models. There is also animal data on heart injury, corneal injury, and liver scarring. Of note, although there is data across independent groups, the majority of the papers are by Allan Goldstein, who is a co-founder of a company called RegeneRx, that owns the rights to develop Tβ4 therapeutically. There have been some human trials of Tβ4 involving wounds, dry eyes, and heart attack. Although research has been ongoing for roughly 20 years, Tβ4 has still not been FDA-approved for any indication.
There is also a safety concern with both TB-500 and Tβ4. Studies have shown that Tβ4 is overexpressed in cancer cells. It may be that some of the same cell migration and angiogenesis properties that promote wound healing could also promote cancer cell spread.
For TB-500 itself, there is almost no animal data, and zero human data. The animal data is so thin that it’s not worth reviewing. In summary, it looks like the reputation of TB-500 is entirely built on an assumption that it might behave like its parent molecule, that is several times larger, with no data to support that assumption. Although it was used by the equine industry and athletes for trying to improve performance, it doesn’t look like there was any data behind that. It was banned not because it had been proven effective, but because there might be the potential for it to have an effect. In the end, we can’t make any conclusions about the safety or efficacy of TB-500.
Lastly, let’s look at BPC-157.
BPC-157: Red Flags Behind the Research
BPC-157 Peptide Side Effects, Studies, and Safety Concerns
BPC-157 is a 15-amino acid peptide derived from a protein found in human gastric juice. It is not known exactly what its molecular target is, but it has been shown in lab testing to upregulate some enzymes and growth factors. It is not FDA-approved for any indication. Research has focused on the effects that it has on pathways that are felt to be involved in healing, such as tendon fibroblast migration, endothelial cell angiogenesis, and vasomotor tone. Most of the studies have been done in animals (primarily rodents), and show various findings such as promoting tendon fibroblast migration, for example, or accelerating the healing of burn wounds. Human data is remarkably sparse. One concern about BPC-157 is that the overwhelming majority of the studies on BPC-157 originate from a single research group in the University of Zagreb, Croatia. The data from this research is mostly inaccessible. Many of the core original research articles are published in Bentham Science journals, behind a paywall. Bentham has been characterized by some researchers as a predatory publisher, with claims that it has lax peer review, and questionable editorial practices.
One study worth mentioning is a 2011 study by Chang et al. from Taiwan, published in the Journal of Applied Physiology. This is notable because it’s one of the few BPC-157 studies done by a group outside of Zagreb. They took tendon tissue from rats and human tendon cells from surgical specimens and showed that BPC-157 increased the migration of tendon fibroblasts (the cells that build tendons) in a dose-dependent manner, and improved cell survival under stress. It’s a well-done study, and it does show a real effect. But it was done in a dish, not in a living animal or human. Showing that cells move faster in a lab doesn’t tell us whether a torn Achilles tendon would heal better in a person.
There is one industry-sponsored Phase 2 clinical trial as of May 2026 that is listed as “recruiting patients” that is looking at whether BPC-157 can speed recovery from an acute hamstring strain. The study design — randomized, double-blind, and placebo-controlled — is exactly the kind that has been missing. But the trial is not being run by an independent academic group, so if this ends up getting published, and if the results are positive, they would need to be replicated independently before drawing any firm conclusions.
There are still multiple red flags about the BPC-157 story. These include that the research is dominated by a single group that has a financial conflict of interest, publications from this group have been in low- to mid-tier journals, there is no raw data availability, they’ve shown almost 100% positive results in studies across a broad range of conditions, and there are no completed or published clinical trial results. In summary, we can’t conclude that BPC-157 is safe or effective.
Putting it all together
What we’re mostly missing, at this point, and what would traditionally be there to help us to evaluate a medical treatment, is good quality evidence on the safety and efficacy of the treatment. This is what would normally happen. If the medication proved safe, and if studies could show efficacy, the chemical would go down the pathway to becoming an FDA-approved medication. “Peptides” have not gone down that path, or some started down it, and fell off of it along the way.
So You’re Still Considering Peptides — Here’s What to Know
Peptide Injections: Gray Market Risks and What Patients Should Know
Is there any possibility, however, that doing a month of daily or regular injections of GLOW stack or Wolverine Stack could help someone’s pulled calf muscle heal faster? I suppose it’s possible. After reading the above, if someone still wanted to do a peptide treatment, what would that look like? They are not available as FDA-approved prescription products at standard pharmacies. Physicians can order them from suppliers. As they’re not FDA-approved medications, they are usually labeled as “For Research Use” only. This is what is called the gray market. One important concern with gray-market peptides is that because they are not manufactured under the same regulatory standards as FDA-approved medications, there is a real risk of contamination, incorrect dosing, or mislabeled products — meaning that what’s in the vial may not be exactly what’s on the label. The FDA doesn’t regulate physicians; that is the purview of state medical boards. Physicians may use some non-FDA-approved substances in limited circumstances, but this is legally and medically complex.
Either way, here we are! They are being produced, distributed, and administered to patients outside of any formal regulatory framework. There are several places locally where someone could make an appointment, discuss the doses, and start a treatment. One additional caveat is worth mentioning. How would someone know what dose to use? I suppose most clinics are doing what other clinics are doing… but what is that based on?
The Regulatory Landscape Is Shifting Fast
FDA and Peptide Therapy Regulations: What’s Changing in 2026
As a timely update, JAMA published an article in May 2026 showing just how quickly this landscape is changing. In April 2026, the FDA removed a dozen gray-market peptides from a list of substances that had raised significant safety concerns. That change was not based on new evidence showing that these peptides are safe or effective. The FDA’s Pharmacy Compounding Advisory Committee is now scheduled to meet in July 2026 to discuss whether compounding pharmacies should be allowed to make several of these peptides, including BPC-157 and TB-500. There is also interest in allowing some peptides to be sold as dietary supplements. At the same time, the FDA is moving to restrict compounding of FDA-approved GLP-1 medications like semaglutide and tirzepatide. So the regulatory environment is very much in flux, and it’s worth keeping an eye on.
The above is a closer look at 3 commonly used peptides. This is a small subset of what is out there, and I can’t speak to all of the available peptides. My research so far, however, is following the trend of “not enough data to recommend.” We do respect that in spite of the lack of data, some patients are willing to accept the risk-benefit ratio of peptide therapy. We are simply here to provide information and counseling. If a patient is getting treatments outside of our clinic, we would like to be involved in helping them with their decisions, and reviewing their progress with them along the way.
Our Verdict: Hope Is Understandable, But Caution Is Warranted
Are Anti-Aging Peptides Worth It? A Physician’s Final Assessment
We started with the question of “What do we think of peptides?” I tried to make this article unbiased and informative. I think our answer is a little different after this review. It’s not simply that we have no information. There is information out there. The problem is that we still do not know whether these peptides are safe or effective. The stories behind their discovery and development also give us little reason to assume that they will work as claimed. I wish I could say otherwise, as the goals of improved healing and youth are deeply understandable. For now, however, I think we should remain focused on a healthy lifestyle: regular exercise, a healthy diet, adequate sleep, low stress, and all of the other things we know are associated with living and aging well.
Please note: This article is for informational and educational purposes only, and is not intended to be medical advice. It does not constitute an endorsement or recommendation of any peptide treatment. As always, please discuss any treatments you are considering with your physician.

